Chapter 8. – Creating Safety: When Violence & Abuse Are Part of the Picture
*If you know that a sex offender or a person who has been convicted of a dangerous crime against children will be around your child, the co-parent must be notified immediately.
What is Domestic Violence?
Domestic violence, child abuse, and child neglect are a feature of family life for many in the United States. For some, these events are unique to the period leading up to and during the separation or divorce. For others, a long history of violence, abuse or neglect convinces one or both parents that a separation or divorce is necessary. Physical violence, threats of violence, sexual assault, and child abuse are illegal. Specific definitions of domestic violence vary from state to state. But federal laws say it is illegal to injure—or threaten to injure—anyone related by blood or marriage, or with whom you are living together or are in an intimate relationship. This is true regardless of your cultural or religious heritage, citizenship status, or personal beliefs about discipline or the proper relationship between husbands and wives.
Domestic violence constitutes the willful intimidation, assault, battery, sexual assault, or other abusive behavior perpetrated by one family member, household member, or intimate partner against another. In most state laws addressing domestic violence, the relationship necessary for a charge of domestic assault or abuse generally includes a spouse, former spouse, persons currently residing together, or those who have resided together within the previous year, or persons who share a common child.
Victims of violence should understand that ignoring abuse will not make it stop. Abuse becomes more serious with time, and victims must realize that an abusive relationship is unhealthy and unsafe. Also, remember that a victim of domestic violence may be either male or female. Children can also be victims—physically, emotionally, or both.
The CDC has noted from survey data, domestic violence is a public health concern that may involve as many as 1 in 4 women and nearly 1 in 10 men have experienced contact sexual violence, physical violence, and/or stalking by an intimate partner during their lifetime. These numbers translate to over 43 million women and 38 million men experienced psychological aggression by an intimate partner in their lifetime.
To read more about the CDC’s finding, please the article found below.
https://www.cdc.gov/intimate-partner-violence/prevention/index.html
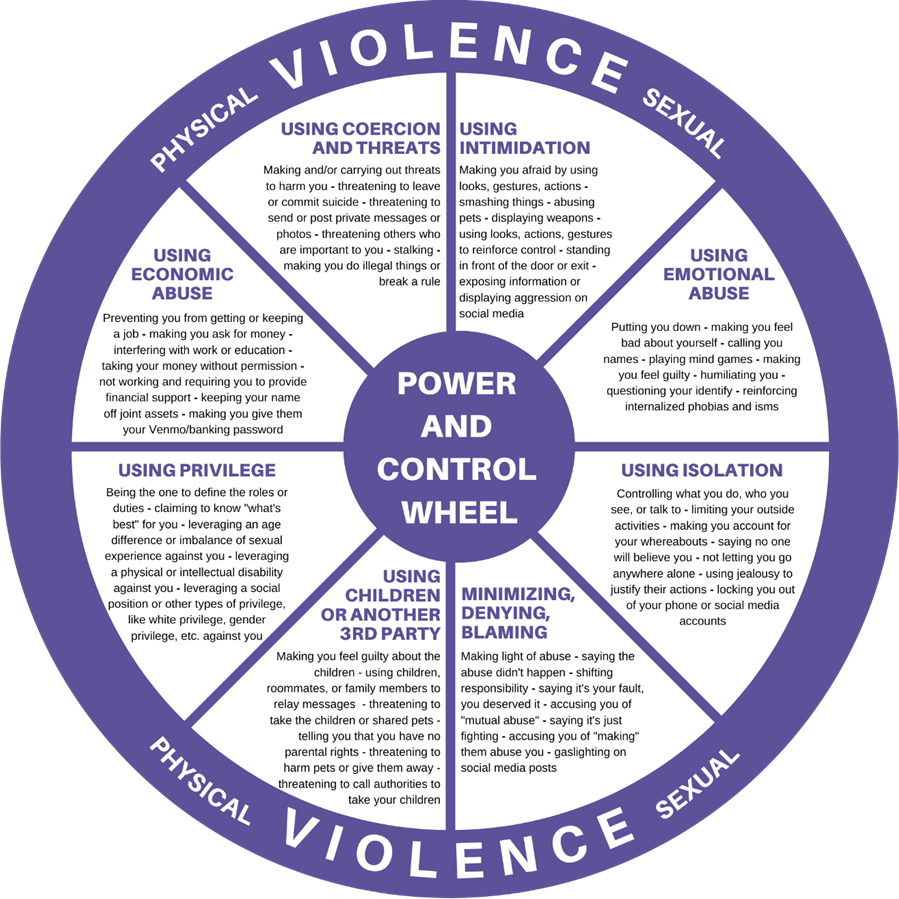
The National Center for Victims of Crime describes the following behaviors as indicative of an abusive personality prone to domestic violence:
- Intimidation: certain looks, gestures, or actions; smashing things; destruction of property or hurting pets; brandishing weapons.
- Emotional Abuse: making the victim feel guilty; calling the victim names; embarrassing, humiliating, or demeaning the victim; playing mind games; telling the victim they are crazy; doing or saying things that make the victim feel that they are crazy.
- Isolation: keeping the victim from going places like visiting family or friends, attending social groups, etc.; listening to phone conversations or opening personal mail; following the victim around and/or questioning them about their whereabouts; using jealousy to justify actions.
- Minimizing, denying, and blaming: making light of the abuse, saying it wasn’t that bad; denying the abuse happened; saying the abuse was the victim’s fault.
- Excessive domination: acting like the master of the house; treating the victim like a servant; making all the big decisions; defining the victim’s role/job; patronizing or in any other way treating the victim like a child, not as an equal adult.
- Economic abuse: preventing the other parent from working outside the home; making them ask for money; limiting money; making them account for all expenditures; not allowing them access to information about family finances.
- Using children: making the victim feel guilty about their parenting skills; making the victim responsible for all the children’s misbehavior or mistakes; undermining the victim’s authority and effectiveness with the children through criticism; telling the children that the victim is stupid or dumb—can’t do anything right; threatening to take the children away or kill them; telling the victim that the Department of Child and Family Services will take the children away.
- Coercion and threats: threatening to take the children away; threatening to destroy property; threatening to harm family or friends; making physical threats and/or actions toward the victim; threatening to leave the victim; threatening to commit suicide.
What are the effects of domestic violence on children?
Domestic violence, child abuse and neglect, and substance abuse represent severe family stressors that fundamentally alter children’s developmental trajectories and create profound challenges for effective co-parenting. Unlike the typical conflicts and stresses associated with separation and divorce, these issues involve safety risks, potential trauma, and patterns of harm that require specialized intervention and often court oversight. For parents in especially challenging co-parenting relationships, understanding the complex dynamics of these issues is essential—whether you are a survivor working to protect yourself and your children, a person who has engaged in harmful behaviors and is working toward change, or a parent trying to navigate co-parenting with someone whose behaviors create ongoing risk. The impact of these issues extends far beyond the immediate harm; they shape children’s neurodevelopment, attachment patterns, emotional regulation capacities, and long-term mental and physical health outcomes in ways that parents must understand to effectively support their children’s recovery and resilience.
Domestic violence—which encompasses physical violence, sexual abuse, emotional and psychological abuse, economic control, coercive control, and intimidation—creates a family environment characterized by fear, unpredictability, and the systematic undermining of one partner’s autonomy and safety. Children exposed to domestic violence, even when not directly physically harmed themselves, experience what researchers term “adverse childhood experiences” (ACEs) that have documented effects on brain development, stress response systems, and long-term health. These children often exhibit symptoms similar to direct abuse victims: hypervigilance, difficulty with emotional regulation, anxiety, depression, behavioral problems, and challenges with trust and attachment. The traditional co-parenting model—which assumes two relatively equal parents who can communicate, negotiate, and collaborate around their children’s needs—fundamentally doesn’t apply in domestic violence cases. The power and control dynamics that characterized the abusive relationship don’t simply end with separation; in fact, the period during and after separation is often the most dangerous time for domestic violence victims. Abusive partners frequently use custody disputes, parenting time exchanges, and communication about children as ongoing opportunities to harass, control, intimidate, or harm their former partners. This means that survivors may need parallel parenting arrangements with minimal contact, highly structured exchanges in safe locations, supervision of parenting time, and clear boundaries that prevent the abuser from using co-parenting as a vehicle for continued abuse.
Child abuse and neglect create their own devastating impacts on children’s development and present unique challenges for co-parenting arrangements. Physical abuse, sexual abuse, emotional abuse, and neglect all interfere with children’s fundamental needs for safety, consistent nurturing, and predictable care. Children who have been abused often struggle with complex trauma responses including dissociation, difficulty trusting adults, extreme behavioral problems or conversely extreme compliance, developmental delays, and mental health challenges. When one parent has abused or neglected the children, the question isn’t simply how to co-parent effectively—it’s whether that parent should have unsupervised access to the children at all, what conditions must be met before contact is safe, and how to structure arrangements that protect children while potentially allowing for a relationship if that serves the child’s best interests and the abusive parent demonstrates genuine change. The non-abusive parent faces the extraordinarily difficult task of supporting their traumatized children through recovery, managing their own emotional responses to their children’s abuse, navigating a legal system that may or may not adequately protect their children, and potentially managing ongoing contact between their children and the person who harmed them if courts order it. This requires understanding trauma-informed parenting, recognizing trauma responses in children, supporting therapeutic interventions, and maintaining appropriate boundaries and safety planning even when court orders require ongoing contact.
Substance abuse adds another layer of complexity and risk to co-parenting dynamics. Parents struggling with alcohol or drug addiction may be unreliable, neglectful, emotionally unavailable, or engage in dangerous behaviors while responsible for children. The unpredictability of addiction—periods of sobriety followed by relapse, promises made and broken, moments of genuine connection undermined by intoxication—creates profound insecurity for children who cannot count on their parent to be consistently safe and present. Children of parents with substance abuse issues often take on inappropriate caretaking roles, experience parentification, develop their own mental health and substance abuse issues, and struggle with anxiety about their parent’s safety and wellbeing. For the co-parent dealing with an addicted former partner, the challenges include determining when supervised visitation is necessary, how to verify sobriety, whether and how to discuss the other parent’s addiction with children, managing children’s disappointment and hurt when the addicted parent fails to show up or appears intoxicated, and navigating the complex emotions of hoping for recovery while protecting children from ongoing harm. Substance abuse frequently co-occurs with domestic violence and child neglect, creating compound risks that require particularly careful assessment and management.
Understanding these issues at a sophisticated level means recognizing several critical concepts. First, the cycle of violence and the pattern of abuse escalation and remission mean that periods of calm or apology don’t indicate that abuse has ended—without significant intervention and genuine change, abusive patterns typically continue and often worsen. Second, children’s loyalty to and love for an abusive or neglectful parent doesn’t mean the abuse wasn’t harmful or that protection isn’t needed—children can simultaneously love a parent and be harmed by that parent’s behavior. Third, false allegations of abuse do occur in custody disputes, but the majority of allegations are substantiated or at minimum represent genuine concerns, and the fear of false allegations should never prevent appropriate reporting and protection of children at risk. Fourth, effective intervention for domestic violence, child abuse, and substance abuse requires specialized treatment and demonstrated behavioral change over time—anger management classes are insufficient for domestic violence, parenting classes alone don’t address child abuse, and simply attending AA meetings doesn’t ensure recovery from addiction. Fifth, survivors of domestic violence and children who have experienced abuse or neglect often require specialized therapeutic support to process trauma, develop safety awareness, and build healthy relationship patterns—recovery is possible but requires appropriate, trauma-informed intervention.
For parents in high-conflict co-parenting relationships involving these serious issues, the practical implications of understanding these dynamics include knowing when to seek protective orders and how to enforce them, understanding the difference between high-conflict co-parenting and co-parenting in the context of abuse (and why strategies appropriate for one are inappropriate or dangerous for the other), learning parallel parenting techniques that minimize contact while maintaining children’s access to both parents when safe, recognizing trauma responses in children and accessing trauma-informed therapeutic support, documenting concerning behaviors and safety risks for court purposes, developing safety plans for exchanges and communication, understanding the role of supervised visitation and reunification therapy when appropriate, advocating effectively within the court system for arrangements that prioritize safety, supporting children’s relationships with a problematic parent when possible while maintaining appropriate boundaries and protections, and recognizing signs of relapse or escalating risk that require immediate intervention. Parents must also understand their own healing process—survivors need support to process their own trauma and develop healthy relationship patterns, while parents who have engaged in harmful behaviors must take responsibility for change, complete appropriate treatment programs, demonstrate sustained behavioral change, and understand that rebuilding trust and relationships takes significant time and may not always be possible depending on the severity of harm and children’s needs.
Options for victims of domestic violence
- Contact a local domestic-violence program. These programs are in many communities around the country and can provide counseling and support groups; information about legal options, the criminal justice system, and social services; shelter; attorney referrals; vocational counseling; safety planning; and case advocacy. Programs will assist victims regardless of their decision to stay in the relationship or leave it..
- Create a comprehensive safety plan. With assistance from a victim-service professional, victims should create an individualized plan for safety in all situations, including a checklist of necessary items to take when leaving an abusive situation.
- Consider legal options. Domestic Violence Advocates are available the Downtown, Southeast, Northwest and Northeast Protective Order Center locations. Advocates are available to speak to victims regarding questions concerning domestic violence and the process to obtain an Order of Protection or Injunction Against Harassment. They can assist victims in obtaining a 911 emergency cell phone; and refer victims to other agencies and organizations that can help with shelter and counseling. In addition, Advocates can accompany individuals to court to get an Order of Protection or Injunction Against Harassment, or other proceedings related to domestic violence. Advocates cannot provide legal advice.
The Department of Health and Human Services website states that “more than 15 million children in the United States live in homes in which domestic violence has happened at least once. These children are at greater risk for repeating the cycle as adults by entering into abusive relationships or becoming abusers themselves. For example, a boy who sees his mother being abused is 10 times more likely to abuse his female partner as an adult. A girl who grows up in a home where her father abuses her mother is more than six times as likely to be sexually abused as a girl who grows up in a non-abusive home” (https://www.womenshealth.gov/relationships-and-safety/domestic-violence/effects-domestic-violence-children).
The article goes on to say that you can help your children by:
- Helping them feel safe. Children who witness or experience domestic violence need to feel safe. Consider whether leaving the abusive relationship might help your child feel safer.
- Talking to them about their fears. Let them know that it’s not their fault or your fault.
- Talking to them about healthy relationships. Help them learn from the abusive experience by talking about what healthy relationships are and are not. This will help them know what is healthy when they start romantic relationships of their own.
- Talking to them about boundaries. Let your child know that no one has the right to touch them or make them feel uncomfortable, including family members, teachers, coaches, or other authority figures. Also, explain to your child that he or she doesn’t have the right to touch another person’s body, and if someone tells them to stop, they should do so right away.
- Helping them find a reliable support system. In addition to a parent, this can be a school counselor, a therapist, or another trusted adult who can provide ongoing support. Know that school counselors are required to report domestic violence or abuse if they suspect it.
- Getting them professional help. Cognitive behavioral therapy (CBT) is a type of talk therapy or counseling that may work best for children who have experienced violence or abuse. CBT is especially helpful for children who have anxiety or other mental health problems as a result of the trauma. During CBT, a therapist will work with your child to turn negative thoughts into more positive ones. The therapist can also help your child learn healthy ways to cope with stress.
Resource PDF link to talk to your child about Domestic Violence found below:
How can I get help in an emergency?
**Immediately dial 911 and request help from the police
Protection Orders
Protection Orders, also called Restraining Orders, are orders to stop specific acts against everyone named in the restraining order as a “Protected Person.” Some of the things that the restrained person can be ordered to:
*Stop contacting, harassing, injuring, intimidating, molesting, threatening, touching, stalking, sexually assaulting or abusing any Protected Person;
*Stop entering or remaining on premises, or coming within a specified distance of a Protected Person or premises;
*Stop taking, transferring, concealing, harming, disposing of, or threatening harm to an animal owned, possessed, leased, kept, or held by a Protected Person; or the court can grant such other relief as the court deems appropriate. C.R.S. 13-14-105(1)(i).
A Temporary or Permanent Civil Protection Order may be issued against an adult or a juvenile who is ten years of age or older.
For more information and access to forms on how to file for a Protection Order in the state of Colorado, please visit
https://www.coloradojudicial.gov/self-help/getting-protection-order
National domestic-violence centers usually provide:
- A 24-hour crisis line
- Temporary shelter
- Advocacy and counseling for victims
- Advocacy and counseling for the children of victims
- Legal information, court accompaniment, and assistance with restraining orders
- Welfare/economic support
- Support groups for battered women and their children
- Information and referral
- Community education
- Outreach to schools, including education on teen dating violence and support for victims
- Batterers treatment
- Sexual-assault services
Important Phone Numbers for Domestic Violence:
National Domestic Violence Hotline……………………………………..(800) 799-SAFE (7233)
National Domestic Violence Hotline ………………………………….. ..(800) 787-3224 (TTY)
National Coalition Against Domestic Violence………………………….(303) 839-1852
National Resource Center on Domestic Violence………………………(800) 537-2238
National Council on Child Abuse and Family Violence………………..(800) 222-2000
Women in Distress: 24-hour crisis line in English and Spanish………(800)-500-1119
Child Abuse
Abuse means any willful act or threatened act that results in any physical, mental, or sexual injury or harm that causes or is likely to cause the child’s physical, mental, or emotional health to be significantly impaired. Abuse of a child includes acts or omissions. Corporal discipline of a child by a parent or legal custodian for disciplinary purposes does not in itself constitute abuse when it does not result in harm to the child. The legal definition of a child is any person under the age of eighteen.
Any person who knows or has reasonable cause to suspect child abuse, abandonment, or neglect by a person responsible for a child’s welfare is required to report that information to the state’s toll-free hotline, an appropriate law-enforcement agency, or (in the case of a child’s death), the medical examiner responsible for the city, town, county, or other area where the death occurred.
Children Exposed to Violence
- Psychological health: depression, anxiety, post-traumatic stress disorder, isolation, shame, fear, guilt, and low self-esteem
- Physical health outcomes: poor overall health, have illnesses requiring medical attention, attempt suicide, or be involved in self-injury. Exposure to child abuse and neglect has profound effects on brain development and cognition.
- Academic difficulties and failure: Exposure to violence increases the risk that children will drop out of school or do more poorly in school
- Behavioral problems: substance abuse or dependence, teen pregnancy, aggression, conduct disorder, delinquency, and violence, including dating violence and intimate partner violence
- Delinquency and offending: Seventy percent of youth in residential placement had some type of past traumatic experience, with 30 percent having experienced frequent and/or injurious physical and/or sexual abuse
Other Kinds of Child Maltreatment
Abandonment is a situation where the parent, legal custodian, or the caregiver responsible for a child’s welfare, although able to care for the child, doesn’t provide for the child’s support and makes no effort to communicate with the child—legally, this is a willful rejection of parental obligations. Token or inadequate efforts to support or communicate with the child may result in a court declaring the child to be abandoned.
Mental injury means substantially decreased ability to function intellectually or psychologically within the normal range of performance and behavior.
Neglect occurs when a child is deprived of necessary food, clothing, shelter, or medical treatment, or when a child is permitted to live in an environment where such deprivation or environment significantly impairs or threatens to impair the child’s physical, mental, or emotional health.
Harm to a child’s health or welfare can occur when any person inflicts upon the child (or allows to be inflicted) physical, mental, or emotional injury. In determining whether harm has occurred, the following factors are considered: the child’s age; any prior history of injuries to the child; the location of the injury on the child’s body; the number of injuries; and the type of trauma inflicted.
Recognizing Child Abuse and Neglect: Signs and Symptoms The following material is reproduced with permission of the National Clearinghouse on Child Abuse and Neglect Information (2003).
The first step in helping abused or neglected children is learning to recognize the signs of child abuse and neglect. The presence of a single sign does not prove child abuse is occurring in a family; however, when these signs appear repeatedly or in combination, you should take a closer look at the situation and consider the possibility of child abuse.
If you do suspect a child is being harmed, reporting your suspicions may protect the child and get help for the family. Contact your local child-protective services agency or police department. For more information about where and how to file a report, call the Childhelp USA® National Child Abuse Hotline (1-800-4-ACHILD).
Please watch video from the CDC explaining Child Abuse and Neglect
https://www.cdc.gov/child-abuse-neglect/about/index.html
Recognizing Child Abuse
The following signs may signal the presence of child abuse or neglect.
The Child:
- Shows sudden changes in behavior or school performance;
- Has not received help for physical or medical problems brought to the parents’ attention;
- Has learning problems that cannot be attributed to specific physical or psychological causes;
- Is always watchful, as though preparing for something bad to happen;
- Lacks adult supervision;
- Is overly compliant, an overachiever, or too responsible; or
- Comes to school early, stays late, and does not want to go home.
The Parent:
- Shows little concern for the child, rarely responding to the school’s requests for information, for conferences, or for home visits;
- Denies the existence of—or blames the child for—the child’s problems in school or at home;
- Asks the classroom teacher to use harsh physical discipline if the child misbehaves;
- Sees the child as entirely bad, worthless, or burdensome;
- Demands perfection or a level of physical or academic performance the child cannot give; or
- Looks primarily to the child for care, attention, and satisfaction of emotional needs.
The Parent and Child:
- Rarely touch or look at each other;
- Consider their relationship entirely negative; or
- State that they do not like each other.
None of these signs taken alone proves that child abuse is present in a family. But when these signs appear repeatedly or in combination, there is the possibility of child abuse.
Types of Abuse
The following are some signs often associated with physical abuse, neglect, sexual abuse, and emotional abuse. It is important to note, however, these types of abuse are more typically found in combination than alone. A physically abused child, for example, is often emotionally abused as well, and a sexually abused child also may be neglected.
Signs of Physical Abuse
Consider the possibility of physical abuse when the child:
- Has unexplained burns, bites, bruises, broken bones, or black eyes;
- Has fading bruises or other marks noticeable after an absence from school;
- Seems frightened of the parents and protests or cries when it is time to go home from school;
- Shrinks at the approach of adults; or
- Reports injury by a parent or another adult caregiver
Consider the possibility of physical abuse when the parent or adult caregiver:
- Offers conflicting, unconvincing, or no explanation for the child’s injury;
- Describes the child as ‘evil,’ or in some other very negative way;
- Uses harsh physical discipline with the child; or
- Has a history of abuse as a child.
Signs of Neglect
Consider the possibility of neglect when the child:
- Is frequently absent from school;
- Begs or steals food or money from classmates;
- Lacks needed medical or dental care, immunizations, or glasses;
- Is consistently dirty and has severe body odor;
- Lacks sufficient clothing for the weather;
- Abuses alcohol or other drugs; or
- States there is no one at home to provide care.
Consider the possibility of neglect when the parent or other adult caregiver:
- Appears to be indifferent to the child;
- Seems apathetic or depressed;
- Behaves irrationally or in a bizarre manner;
- Is abusing alcohol or other drugs; or
- States that there is no one at home to provide care
- Consider the possibility of neglect when the parent or other adult caregiver:
- Appears to be indifferent to the child;
- Seems apathetic or depressed;
- Behaves irrationally or in a bizarre manner; or
- Is abusing alcohol or other drugs.
Signs of Sexual Abuse
Consider the possibility of sexual abuse when the child:
- Has difficulty walking or sitting;
- Suddenly refuses to change for gym or to participate in physical activities;
- Reports nightmares or bedwetting;
- Experiences a sudden change in appetite;
- Demonstrates bizarre, sophisticated, or unusual sexual knowledge or behavior;
- Becomes pregnant or contracts a venereal disease, particularly if under age 14;
- Runs away; or
- Reports sexual abuse by a parent or another adult caregiver.
Consider the possibility of sexual abuse when the parent or other adult caregiver:
- Is unduly protective of the child or severely limits the child’s contact with other children, especially of the opposite sex;
- Is secretive and isolated; or
- Is jealous or controlling with family members.
Signs of Emotional Maltreatment
Consider the possibility of emotional maltreatment when the child:
- Shows extremes in behavior, such as overly compliant or demanding behavior, extreme passivity, or aggression;
- Is either inappropriately adult (parenting other children, for example) or inappropriately infantile (frequently rocking or head-banging, for example);
- Is delayed in physical or emotional development;
- Has attempted suicide; or
- Reports a lack of attachment to the parent.
Consider the possibility of emotional maltreatment when the parent or other adult caregiver:
- Constantly blames, belittles, or berates the child;
- Is unconcerned about the child and refuses to consider offers of help for the child’s problems; or
- Overtly rejects the child.
This fact sheet was adapted, with permission, from Recognizing Child Abuse: What Parents Should Know. Prevent Child Abuse America, © 2003.
What are the consequences of filing a false child-abuse report?
In some instances, a parent may be tempted to file a false child-abuse report against the child’s mother or father. This is usually done to gain some kind of advantage over the other parent. You should never resort to this, and parents are strongly discouraged from this type of action. According to most state statutes, a person who knowingly and willfully makes a false report of child abuse, abandonment, or neglect, or who advises another to make a false report, is guilty of a felony in the third degree. However, anyone making a report who is acting in good faith is immune from liability.
Anger Management Skills
Anger management in the context of high-conflict co-parenting relationships requires understanding that anger itself is not the problem—it’s a natural, legitimate emotional response to perceived injustice, betrayal, loss, and the profound disruption of separation or divorce. The challenge isn’t eliminating anger but rather developing the capacity to experience anger without allowing it to drive destructive behaviors that harm your children, damage your co-parenting relationship further, or undermine your credibility in legal proceedings. Many parents going through difficult separations experience intense, persistent anger that feels entirely justified given their circumstances—perhaps their ex-partner was unfaithful, financially irresponsible, neglectful of the children, or behaved in ways that genuinely warrant anger. The sophisticated understanding of anger management recognizes this reality while also acknowledging that regardless of how justified your anger may be, acting on it impulsively through hostile communications, retaliatory behaviors, or exposing your children to your rage will ultimately harm the people you’re trying to protect and undermine your own goals. Effective anger management for co-parents involves developing what psychologists call “emotional regulation”—the ability to notice anger arising, understand what’s triggering it, tolerate the uncomfortable physical and emotional sensations that accompany it, and choose a response that aligns with your values and long-term interests rather than providing momentary emotional release.
The neuroscience of anger helps explain why managing it is so difficult, particularly in the context of interactions with a former partner who may know exactly which buttons to push. When you perceive a threat—whether it’s a hostile text from your co-parent, learning they’ve violated an agreement, or witnessing behavior you believe harms your children—your brain’s amygdala triggers a fight-or-flight response before your prefrontal cortex (the rational, decision-making part of your brain) has fully processed the situation. This means you may experience a surge of anger, increased heart rate, muscle tension, and narrowed focus on the perceived threat within milliseconds, while the part of your brain capable of perspective-taking, consequence-consideration, and thoughtful response takes longer to come online. This physiological reality explains why you might send an angry text or make a hostile comment that you immediately regret—your emotional brain responded before your thinking brain could intervene. Effective anger management strategies work with this neurological reality rather than against it. This means building in deliberate pauses between trigger and response—practices like the 24-hour rule before responding to inflammatory communications, physically removing yourself from triggering situations when possible, using specific techniques to activate your parasympathetic nervous system (deep breathing, progressive muscle relaxation, going for a walk), and developing the self-awareness to recognize your personal early warning signs that anger is escalating before you’ve reached the point where rational decision-making becomes nearly impossible.
Advanced anger management also requires understanding the difference between primary and secondary emotions. Anger is often a secondary emotion that covers or protects us from more vulnerable primary emotions like hurt, fear, grief, shame, or helplessness. When your co-parent shows up late for an exchange again, your immediate anger may actually be covering fear that your children aren’t a priority to them, hurt that your family has dissolved, or helplessness about your inability to control their behavior. When you can identify and acknowledge these underlying emotions—even just to yourself—you often find that the anger becomes more manageable and you can respond more effectively to the actual situation. This doesn’t mean sharing these vulnerable emotions with your co-parent, particularly in a high-conflict relationship where emotional vulnerability might be used against you. Rather, it means doing the internal work to understand what’s really driving your anger so you can address your actual needs rather than simply reacting to surface triggers. This might involve journaling, therapy, trusted conversations with friends or support groups, or other practices that help you process the complex emotions of divorce and develop more sophisticated emotional awareness.
Practical anger management strategies for high-conflict co-parenting include developing a personal “anger action plan” that you create when you’re calm and can think clearly, which you then implement when you’re triggered. This plan might include specific self-soothing techniques you’ll use (breathing exercises, physical exercise, calling a supportive friend, listening to specific music), a commitment to delay responses when you’re emotionally activated (the 24-hour email rule, drafting but not sending responses, using templates for necessary communications), environmental strategies that reduce triggers (using email rather than phone calls, scheduling exchanges in public locations, using a third party for transitions), and accountability measures (having a trusted friend review communications before you send them, working with a therapist on emotional regulation, using apps that delay message sending). It also means developing realistic expectations—accepting that your co-parent may continue behaviors that anger you, that you cannot control or change them, and that your energy is better spent on what you can control: your own responses, your relationship with your children, and creating stability in your own household. Some parents find it helpful to reframe co-parenting communications as “business transactions” requiring professional courtesy but not personal investment—you wouldn’t scream at a difficult customer or colleague, even if their behavior frustrated you, because it would be unprofessional and counterproductive. Applying this same standard to co-parenting communications can help create emotional distance that makes anger management easier. Finally, anger management requires self-compassion and realistic expectations for yourself—you will sometimes fail at managing your anger effectively, you will occasionally say or do things you regret, and this doesn’t mean you’re a failure or a bad parent. What matters is that you recognize these moments, take responsibility for them, make amends when appropriate, and continue working on developing better skills. The goal isn’t perfection but rather gradual improvement in your capacity to experience intense anger without allowing it to drive behaviors that ultimately harm you and your children.
The Impact of Trauma on Brain Development and What to Do About it
The effects of chronic, overwhelming stress and trauma on children’s development is under constant scrutiny. Parents, educators, clinicians, mental health workers and law enforcement struggle to understand the impacts of trauma on brain development in a concrete and tangible way.
Collaborative Problem Solving (CPS) is a practical, evidence-based process that all adults can follow in any setting to ensure trauma-informed intervention. CPS has been used effectively across systems to provide concrete strategies needed to provide clear guideposts for adults to use in order to engage children in problem solving discussions. This helps build relationships with the children while fostering a relationship that develops flexibility, problem solving, and emotion regulation skills.
Facilitating brain change is not about erasing old associations in the brain resulting from trauma, but about creating new neural pathways. Exposing children repeatedly to small, digestible doses of novel experiences with a different, more positive emotional quality to them creates these pathways. Once a child is regulated, CPS then helps the adult relate to the child by sharing their adult concerns. Finally, the child is then asked to reason with the adult to collaborate and brainstorm solutions. The entire process is built to help adults expose children to these small, digestible doses of “good stress” needed to foster brain change.
Core Components of Adult Trauma-Informed Problem Solving
- Establish Safety First: Ensure physical and emotional safety before attempting to solve problems, as fear disrupts the brain’s ability to think clearly.
- Self-Regulation: Use techniques to calm the nervous system (e.g., deep breathing, grounding) to move from a threat-response state to a calm state where the prefrontal cortex can function.
- Shift Perspective (Curiosity over Judgment): Approach behavioral issues with curiosity regarding underlying causes rather than immediate punitive judgment.
- Identify Triggers: Recognize specific situations, words, or actions that trigger trauma responses.
- Collaborative Approach: Work with the individual to find solutions rather than imposing them, which fosters empowerment and choice.
Important Phone Numbers for Child Abuse
Missing Children Info…………………………………………………………1-800-342-0821
Runaway Helpline……………………………………………………….……1-800-621-4000
Child Abuse Hotline ………………………………………………..………..1-800-962-2873
Child Support Hotline………………………………………………………..1-800-622-KIDS
National Center for Missing Children…………………………………… 1-800-843-5678
Choosing a Mental-Health Professional
One of the hurdles in finding a qualified therapist to help your family is wading through the various kinds of mental-health professionals. At a minimum, you will want to seek a professional who holds a license in marriage and family therapy, mental-health counseling, or social work. These professionals will have either a master’s degree or a doctorate. Keep in mind, however, that the individual therapist is always more important than their degree, certification, licensure, or other qualification. Most of the professional’s expertise will come as they specialize in their work. You will want to make sure that a professional you choose has experience with divorce issues and helping families in transition.
Preventing Adverse Childhood Experiences
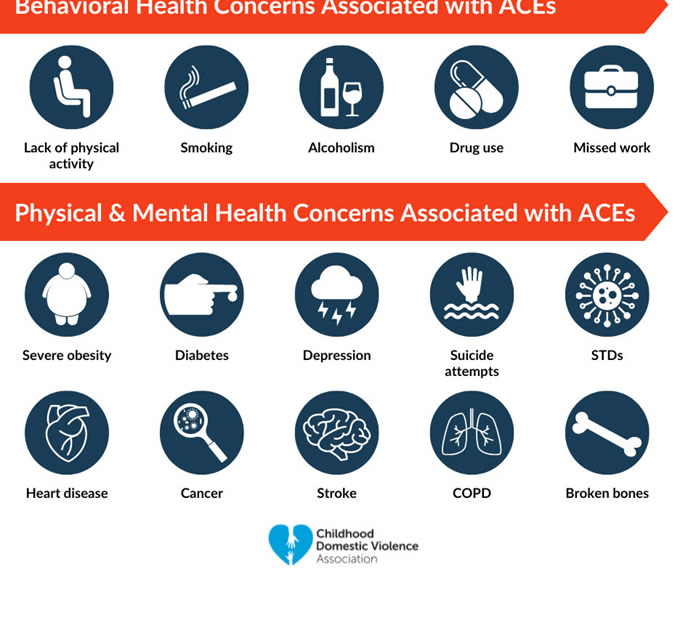
The Adverse Childhood Experiences (ACE) Study, conducted by the Centers for Disease Control and Prevention and Kaiser Permanente in the 1990s, represents one of the most significant pieces of research in understanding how childhood trauma affects long-term health and wellbeing. The study surveyed over 17,000 adults about their childhood experiences across ten categories of adversity: physical abuse, sexual abuse, emotional abuse, physical neglect, emotional neglect, witnessing domestic violence, household substance abuse, household mental illness, parental separation or divorce, and incarcerated household members. The findings were stunning and have fundamentally changed how we understand childhood trauma. The research demonstrated a powerful, dose-response relationship between the number of adverse experiences a person had in childhood and negative outcomes in adulthood, including chronic diseases (heart disease, cancer, lung disease, liver disease), mental health problems (depression, anxiety, suicide attempts), substance abuse, risky behaviors, and even early death. Perhaps most remarkably, the study found that ACEs are incredibly common—about two-thirds of participants reported at least one ACE, and one in eight reported four or more. For parents going through separation or divorce, the ACE study provides critical context: parental separation is itself considered an adverse childhood experience, which means divorce alone contributes to your child’s ACE score. However, it’s not the divorce itself that causes the most harm—it’s the associated experiences like witnessing violence between parents, living with a parent with untreated mental illness or addiction, experiencing abuse or neglect, or being caught in ongoing high conflict. This understanding should motivate parents to minimize additional adversity during and after divorce, protect children from conflict and adult burdens, address their own mental health and substance issues, and create as much stability and safety as possible.
The mechanism by which ACEs cause these long-term negative outcomes involves the impact of chronic stress and trauma on the developing brain and body’s stress response systems. When children experience chronic stress—whether from abuse, neglect, household dysfunction, or ongoing exposure to frightening or unpredictable situations—their developing brains and bodies adapt to an environment of threat. The brain’s amygdala (threat detection center) becomes hyperactive and oversized, the prefrontal cortex (responsible for executive functioning, emotional regulation, and decision-making) develops more slowly or differently, and the hippocampus (involved in memory and learning) may be smaller. The body’s stress response system, the hypothalamic-pituitary-adrenal (HPA) axis, becomes dysregulated from being chronically activated. These aren’t just temporary states—they represent actual physical changes in brain structure, neural pathways, and biological stress response systems that can persist throughout life. Children living in chronic stress states effectively have their brains and bodies calibrated for survival in threatening environments. This adaptation, while protective in genuinely dangerous situations, becomes maladaptive when it persists into adulthood and causes hypervigilance, difficulty with emotional regulation, impaired decision-making, relationship problems, and vulnerability to mental health and substance abuse issues. The stress response system that’s been activated repeatedly becomes sensitized, meaning it fires more easily and intensely in response to stressors, and takes longer to return to baseline. Over time, this chronic activation of stress systems contributes to inflammation, immune dysfunction, and the chronic diseases documented in the ACE study.
For parents navigating separation and divorce, understanding the neurobiology of traumatic stress has profound implications for how they approach co-parenting and protecting their children. First, it underscores why minimizing children’s exposure to parental conflict is so critical—witnessing ongoing hostility, aggression, or violence between parents literally changes children’s developing brains in ways that increase vulnerability to problems throughout life. Second, it explains why children exposed to high-conflict divorces may exhibit behavioral problems, academic difficulties, emotional dysregulation, or physical complaints—these aren’t character flaws or manipulation, but rather nervous system responses to chronic stress that children cannot control. Third, it highlights the importance of creating environments of safety, predictability, and nurturing care, which actually support healthy brain development and can help buffer against or even reverse some effects of earlier adversity. Parents who understand this neuroscience are better equipped to respond to their children’s stress-related behaviors with compassion rather than punishment, to prioritize creating calm, stable home environments over being the “fun” or permissive parent, and to recognize that their own emotional regulation and mental health directly impact their children’s developing stress response systems. Children learn to regulate their own emotions and stress through co-regulation with calm, attuned caregivers—when parents can maintain their own regulation despite stress, they literally help wire their children’s brains for healthier stress responses. Finally, this understanding should motivate parents to seek appropriate therapeutic support for children showing signs of traumatic stress, to address their own ACEs and trauma that may be affecting their parenting, and to recognize that while they cannot undo the adversity of divorce, they can absolutely influence how much additional adversity their children experience and how well-supported children are in processing and recovering from these experiences. The ACE study’s most hopeful finding is that resilience factors—like having at least one stable, supportive adult relationship—can significantly buffer against negative outcomes even for children with high ACE scores, which means that parents who show up consistently with love, stability, and appropriate boundaries are providing one of the most powerful protective factors available.
Adverse childhood experiences, or ACEs, are potentially traumatic events that occur in childhood (0-17 years). For example: experiencing violence, abuse, or neglect, witnessing violence in the home or community, having a family member attempt or die by suicide.
Also included are aspects of the child’s environment that can undermine their sense of safety, stability, and bonding such as growing up in a household with: substance misuse, mental health problems, instability due to parental separation or household members being in jail or prison.
ACEs are linked to chronic health problems, mental illness, and substance misuse in adulthood. ACEs can also negatively impact education and job opportunities. However, ACEs can be prevented.
How big is the problem?
ACEs are common. About 61% of adults surveyed across 25 states reported that they had experienced at least one type of ACE, and nearly 1 in 6 reported they had experienced four or more types of ACEs.
Preventing ACEs could potentially reduce a large number of health conditions. For example, up to 1.9 million cases of heart disease and 21 million cases of depression could have been potentially avoided by preventing ACEs.
Some children are at greater risk than others. Women and several racial/ethnic minority groups were at greater risk for having experienced 4 or more types of ACEs.
ACEs are costly. The economic and social costs to families, communities, and society totals hundreds of billions of dollars each year.
What are the consequences?
ACEs can have lasting, negative effects on health, well-being, and opportunity. These experiences can increase the risks of injury, sexually transmitted infections, maternal and child health problems, teen pregnancy, involvement in sex trafficking, and a wide range of chronic diseases and leading causes of death such as cancer, diabetes, heart disease, and suicide.
ACEs and associated conditions, such as living in under-resourced or racially segregated neighborhoods, frequently moving, and experiencing food insecurity, can cause toxic stress (extended or prolonged stress). Toxic stress from ACEs can change brain development and affect such things as attention, decision-making, learning, and response to stress.
Children growing up with toxic stress may have difficulty forming healthy and stable relationships. They may also have unstable work histories as adults and struggle with finances, jobs, and depression throughout life. These effects can also be passed on to their own children. Some children may face further exposure to toxic stress from historical and ongoing traumas due to systemic racism or the impacts of poverty resulting from limited educational and economic opportunities.
How Can we Prevent Adverse Childhood Experiences?
ACEs are preventable. Creating and sustaining safe, stable, nurturing relationships and environments for all children and families can prevent ACEs and help all children reach their full potential.
CDC has produced a resource, Preventing Adverse Childhood Experiences (ACEs): Leveraging the Best Available Evidence, to help states and communities take advantage of the best available evidence to prevent ACEs. It features six strategies from the CDC Technical Packages to Prevent Violence.
https://www.cdc.gov/aces/prevention/index.html
Raising awareness of ACEs can help:
Change how people think about the causes of ACEs and who could help prevent them.
Shift the focus from individual responsibility to community solutions.
Reduce stigma around seeking help with parenting challenges or for substance misuse, depression, or suicidal thoughts.
Promote safe, stable, nurturing relationships and environments where children live, learn, and play.
Let’s help all children reach their full potential and create neighborhoods, communities, and a world in which every child can thrive.
Case Study
One of the responsibilities for being a licensed marriage and family therapist is that of being a mandated reporter. It is not a therapist job to prove or uncover if abuse or violence is taking place, but rather to report suspected abuse. Most people know that child abuse is a reportable offense, however many people are unaware that parents abusing one another is also considered child abuse. Regardless of whether parents are abusing one another emotionally, physically, or psychologically (state laws typically don’t distinguish), if children are present that is a reportable offense.
Christine and Michael sought help for their 14-year-old son Ryan. Ryan was acting out in a variety of ways and both parents were concerned about the choices he was making. Initially, Christine brought him in for few sessions and it became apparent to me that there was a pretty intense triangle involving the two parents and Ryan. I asked Christine if she would invite Michael to our third session. She said she would prefer if I called him directly, which I did. As always with couples, when you listen to one of them, you can get pulled to seeing things from their perspective. In the first two sessions, I had had certainly gotten an earful about what a terrible parent Michael was from Christine’s perspective.
As in most cases, when I met with Michael, he had his side of the story that painted Christine as the more guilty party with respect to their problems. In these situations, both parents fail to realize that their behaviors are both contributing to the overall distress that the family is experiencing. Both parents feel like they are doing the right thing and that all the problems can be linked to the behavior of the other parent. The escalating cycles of disagreement between Christine and Michael became screaming matches that degenerated into name-calling. Though they were civilized in my office, they both agreed that the intensity outside of therapy was of concern to them both.
This couple was caught in an escalating cycle of verbal and emotional violence toward one another. Through therapy, they became aware of the destruction this was causing. Even with that insight, they were still not motivated to do anything different. Once I learned about the escalating cycle of intensity, it was apparent to me that a call needed to be made to the child abuse hotline. This is never an easy situation for a therapist because you are jeopardizing the client/therapist relationship. From their perspective, they feel they are reaching out for help so the phone call is unnecessary. On the contrary, licensed mental health professional can lose their license if they fail to report suspected abuse. In this instance, Christine and Michael had given me many examples of when their escalating interactions were in the presence of Ryan, therefore qualifying as child abuse.
I gave this couple the opportunity to make the phone call to the child abuse hotline from my office and with me present. Though they were clearly upset, they did understand my responsibility. They also finally got the understanding of the destructiveness of their behavior. Being faced with having to make such a call for your own behavior can be a very sobering experience. If the therapeutic relationship can be salvaged, and many times it cannot, some very productive work can take place. In this case, Christine and Michael did not see me as the enemy, but rather a professional doing my job.
There are many situations of domestic violence where one partner is oppressing the other, a victim. However, in my experience, it is just as common to have two partners participating in the cycle of domestic abuse.
In the next session, we discussed the visit to their home by the child protective services worker. Both parents recounted the horror of having to answer questions about the quality of their parenting. It created quite a shift for Michael and Christine and it was their wake-up call to begin handling things differently with respect to their son Ryan. They each made themselves responsible to work on conflict resolution and anger management skills. There were going to do this through a combination of individual therapy and reading books on the subject. They both agreed to call timeout when things begin to escalate and they also agreed to cease having any discussions in front of Ryan that could lead to a blow up. Christina and Michael were very motivated clients and they both wanted the best for their son Ryan.